Understanding the Cryptorchid
![]() This section is designed to make the procedure of castration and crytorchidectomy easier to understand. Some oversimplification of the embryology of the testis and the assumption that readers are familiar with anatomical and developmental terminology is required for brevity.
This section is designed to make the procedure of castration and crytorchidectomy easier to understand. Some oversimplification of the embryology of the testis and the assumption that readers are familiar with anatomical and developmental terminology is required for brevity.
The following is not intended to be a detailed discussion of the embryology of male development in the horse, but a simplified version pointing out some important factors in the surgical anatomy of cryptorchid castrations.
For more detailed information, please refer to the selected bibliography at the end of this section.
Anatomy and Anatomical Terminology
![]() The word “cryptorchid” is used to describe any testis that is not in the scrotum. There are three types of cryptorchids.
The word “cryptorchid” is used to describe any testis that is not in the scrotum. There are three types of cryptorchids.
1.![]() Inguinal
Inguinal
2.![]() Abdominal
Abdominal
3.![]() Incomplete
Incomplete
In the normal juvenile or adult male horse the testis is found in the scrotum.
![]() A peritoneal process, the “vaginal tunic” (or just “the tunic”) passes through the inguinal canal and surrounds the blood and nerve supply to the testis, as well as the vas deferens, and surrounds testis and epididymis in the scrotum (The blood vessels are branches of the testicular artery and vein, which leave the caudal aorta and vena cava in the dorsal lumbar region, near the kidney).
A peritoneal process, the “vaginal tunic” (or just “the tunic”) passes through the inguinal canal and surrounds the blood and nerve supply to the testis, as well as the vas deferens, and surrounds testis and epididymis in the scrotum (The blood vessels are branches of the testicular artery and vein, which leave the caudal aorta and vena cava in the dorsal lumbar region, near the kidney).
![]() The inguinal canal in the horse is relatively longer than in other species and runs between a deep and a superficial hole in the body wall. These are called the “internal inguinal ring” and the “external inguinal ring”, respectively.
The inguinal canal in the horse is relatively longer than in other species and runs between a deep and a superficial hole in the body wall. These are called the “internal inguinal ring” and the “external inguinal ring”, respectively.
![]() The external inguinal ring is larger than the internal inguinal ring and is palpable in the groin region, especially with the horse in dorsal recumbency. The internal inguinal ring is smaller and is not palpable from outside the abdomen.
The external inguinal ring is larger than the internal inguinal ring and is palpable in the groin region, especially with the horse in dorsal recumbency. The internal inguinal ring is smaller and is not palpable from outside the abdomen.
![]() The “vaginal ring” is the peritoneal lining of the internal inguinal ring. The “vaginal process” is a conical piece of the peritoneal lining that is attached to the tail of the epididymis by the ligament of the tail of the epididymis and will become the “vaginal tunic” once the epididymis and testis pass through the inguinal canal and exit the abdomen.
The “vaginal ring” is the peritoneal lining of the internal inguinal ring. The “vaginal process” is a conical piece of the peritoneal lining that is attached to the tail of the epididymis by the ligament of the tail of the epididymis and will become the “vaginal tunic” once the epididymis and testis pass through the inguinal canal and exit the abdomen.
Testicular Development and Descent in the Equine Fetus (very simplified!)
![]() The left and right testes each differentiate on the dorsal body wall from the corresponding Wolffian or mesonephric duct next to the primordial kidneys (mesonephros) in the first 5 ½ weeks of fetal development. At this time a chord of mesenchyme, called the “gubermaculum” runs from the caudal pole of the testis and the developing tail of the epididymis to the caudo-ventral body wall. This structure will differentiate into the ligament of the tail of the epididymis, and the vaginal ring itself. These structures are critical in finding and delivering a cryptorchid testis in surgery.
The left and right testes each differentiate on the dorsal body wall from the corresponding Wolffian or mesonephric duct next to the primordial kidneys (mesonephros) in the first 5 ½ weeks of fetal development. At this time a chord of mesenchyme, called the “gubermaculum” runs from the caudal pole of the testis and the developing tail of the epididymis to the caudo-ventral body wall. This structure will differentiate into the ligament of the tail of the epididymis, and the vaginal ring itself. These structures are critical in finding and delivering a cryptorchid testis in surgery.
![]() Between 5 and 8 months of pregnancy the testes lay right next to the developing vaginal ring (to which it is attached by the gubernaculum) and become quite large. In fact, during this period the intra-abdominal fetal testis is as large as that of a full-grown stallion. This increase in size occurs by adding cells inside of the testis and causes the bottom of the organ to approach the internal inguinal ring while the top of the testis remains in contact with the dorsal abdominal wall.
Between 5 and 8 months of pregnancy the testes lay right next to the developing vaginal ring (to which it is attached by the gubernaculum) and become quite large. In fact, during this period the intra-abdominal fetal testis is as large as that of a full-grown stallion. This increase in size occurs by adding cells inside of the testis and causes the bottom of the organ to approach the internal inguinal ring while the top of the testis remains in contact with the dorsal abdominal wall.

Prior to birth, the testes begin to shrink. As they shrink, they pull away from the kidney, while they remain very close to the inguinal canal. Just as they added cells to grow in size, they lose cells to shrink. This process leaves each testis somewhat soft and pliable, which allows it to slip through the internal inguinal ring (vaginal ring) and into the inguinal canal.

Normally, the testis slips into the inguinal canal during a brief period prior to parturition when the internal inguinal ring is widest in its development. During this limited amount of time the testis must shrink enough to pass through the ring. If not one could think of it as having “lost the chance” to enter the canal and is, therefore, “trapped” in the abdomen. In this case the testis will never leave the abdomen unless it is removed surgically.

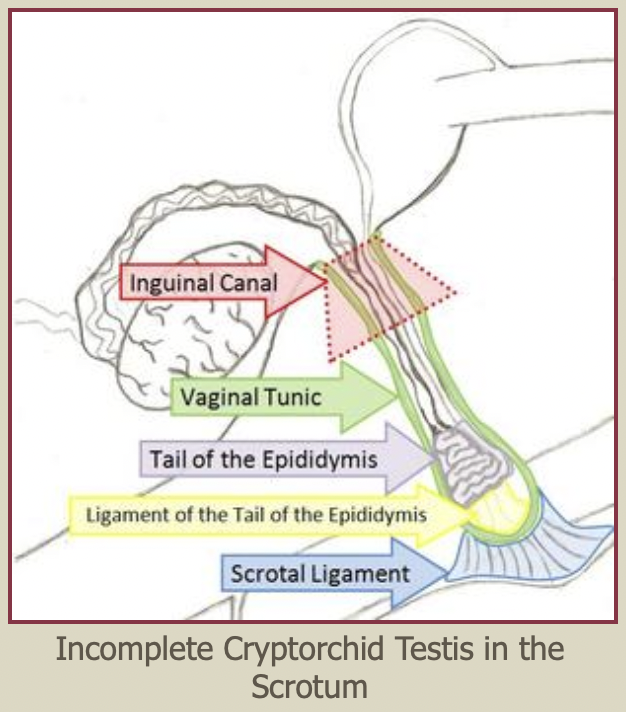
Incomplete Cryptorchid Testis, in the Inguinal Canal

Those that remain in the inguinal canal or do not quite make it to the scrotum will often arrive in the scrotum as the horse matures and the testes enlarge. Horsemen refer to this as the testis “descending,” or “dropping.” The colloquial term for a horse with a testis hidden in the inguinal canal or under the skin outside the scrotum is a “high flanker”.
![]() On the other hand, if the testes are able to slip into the inguinal canal during this time frame (and most of them do) they will eventually migrate subcutaneously to the scrotum (although they may remain in the inguinal canal for some period of time after birth). The vast majority do become scrotal testes, and are removed by routine castration technique.
On the other hand, if the testes are able to slip into the inguinal canal during this time frame (and most of them do) they will eventually migrate subcutaneously to the scrotum (although they may remain in the inguinal canal for some period of time after birth). The vast majority do become scrotal testes, and are removed by routine castration technique.
![]() If the testis does NOT enter the canal (remains in the abdomen), it is most often found just inside the internal inguinal ring. At times the tail of the epididymis enters the inguinal canal unaccompanied by the testis. This is referred to as an “incomplete” cryptorchid. On very rare occasions a testis will remain in the dorsal or caudal abdomen, anywhere from the origin of the testicular arteries and veins in the lumbar region, along the normal pattern of decent in the fetus, to near the internal inguinal ring.
If the testis does NOT enter the canal (remains in the abdomen), it is most often found just inside the internal inguinal ring. At times the tail of the epididymis enters the inguinal canal unaccompanied by the testis. This is referred to as an “incomplete” cryptorchid. On very rare occasions a testis will remain in the dorsal or caudal abdomen, anywhere from the origin of the testicular arteries and veins in the lumbar region, along the normal pattern of decent in the fetus, to near the internal inguinal ring.
Abdominal Cryptorchid Testis

Inguinal Cryptorchids and “High Flankers”
![]() In younger horses with small testes, the cremaster muscle can pull the testis into the external inguinal ring and “hide” it inside the inguinal canal. For this reason, some prefer to wait until horses are older than a year for castration. However, horses cannot pull a testis through the internal inguinal canal and into the abdomen. Inguinal and subcutaneous testes are actually easy to find using good anesthesia technique, patient positioning, and anatomical knowledge.
In younger horses with small testes, the cremaster muscle can pull the testis into the external inguinal ring and “hide” it inside the inguinal canal. For this reason, some prefer to wait until horses are older than a year for castration. However, horses cannot pull a testis through the internal inguinal canal and into the abdomen. Inguinal and subcutaneous testes are actually easy to find using good anesthesia technique, patient positioning, and anatomical knowledge.
The inguinal cryptorchid is the most common presentation and is no more difficult to castrate than a normal testis. Push your hand firmly into the ring. If the testis is in the inguinal canal, it will be expelled superficially and appear as a smooth movable structure under the loose skin between the external inguinal ring and the scrotum.
To find an inguinal or subcutaneous testis:
1.![]() Put the horse into dorsal or semi-dorsal recumbency.
Put the horse into dorsal or semi-dorsal recumbency.
2.![]() Find the easily palpable external inguinal ring in the groin region of the patient. It will be a 3-4 inch slit running in and parallel to the crease between the abdominal wall and the inside of thigh (see figure ).
Find the easily palpable external inguinal ring in the groin region of the patient. It will be a 3-4 inch slit running in and parallel to the crease between the abdominal wall and the inside of thigh (see figure ).
3.![]() Put firm downward pressure into the inguinal canal. If the testis is in the canal it will slide into the subcutaneous space and be readily palpable. Feeling along a line between the external ring and the scrotum will identify subcutaneous testes, as well. Unlike superficial inguinal lymph nodes and fat, a testis is oblong, smooth, and “slippery”.
Put firm downward pressure into the inguinal canal. If the testis is in the canal it will slide into the subcutaneous space and be readily palpable. Feeling along a line between the external ring and the scrotum will identify subcutaneous testes, as well. Unlike superficial inguinal lymph nodes and fat, a testis is oblong, smooth, and “slippery”.
4.![]() If the testis can be manipulated into the scrotum, the castration proceeds by the normal protocol. If the testis cannot be moved to the scrotum, an incision is made over the testis (or over the inguinal canal) and the testis is emasculated as it would be in a routine castration.
If the testis can be manipulated into the scrotum, the castration proceeds by the normal protocol. If the testis cannot be moved to the scrotum, an incision is made over the testis (or over the inguinal canal) and the testis is emasculated as it would be in a routine castration.

Abdominal Cryptorchids
![]() Both the abdominal and incomplete cryptorchid are more difficult cases to handle. Remember: the abdominal cryptorchid testis is ALMOST always found just inside the internal inguinal ring. This is as one would expect from the development and decent of the testis discussed above. Therefore, in the majority of cases the testis can be pulled through the internal inguinal ring and the inguinal canal with a little firm, gentle traction. In the extremely rare instance that the cryptorchid testis is not next to the internal inguinal ring, it may be found at any point along the path followed during normal decent between the lumbar dorsal body wall and the internal inguinal ring.
Both the abdominal and incomplete cryptorchid are more difficult cases to handle. Remember: the abdominal cryptorchid testis is ALMOST always found just inside the internal inguinal ring. This is as one would expect from the development and decent of the testis discussed above. Therefore, in the majority of cases the testis can be pulled through the internal inguinal ring and the inguinal canal with a little firm, gentle traction. In the extremely rare instance that the cryptorchid testis is not next to the internal inguinal ring, it may be found at any point along the path followed during normal decent between the lumbar dorsal body wall and the internal inguinal ring.
The Surgical Approach to an Abdominal Cryptorchid Testis
![]() There area a variety of techniques to finding and removing an abdominal testis in the horse. The following approach has proven effective and safe for field cryptorchid castrations and will be discussed in a series of sequential steps. To be successful, a grasp of the anatomical and developmental aspects of the testis and surrounding structures is essential. Once it has been established that the testis is not in the scrotum, the inguinal canal, or under the skin between these two structures, proceed as follows:
There area a variety of techniques to finding and removing an abdominal testis in the horse. The following approach has proven effective and safe for field cryptorchid castrations and will be discussed in a series of sequential steps. To be successful, a grasp of the anatomical and developmental aspects of the testis and surrounding structures is essential. Once it has been established that the testis is not in the scrotum, the inguinal canal, or under the skin between these two structures, proceed as follows:
1.![]() Establish that the horse is at an adequate plain of anesthesia to allow it to be placed in dorsal recumbency and that it is adequately relaxed. This may require additional xylazine, ketamine, and valium. Glycerol Guaicolate or “Triple Drip” may also be used if a catheter is in place. A good experienced field anesthetist should be in charge of anesthesia.
Establish that the horse is at an adequate plain of anesthesia to allow it to be placed in dorsal recumbency and that it is adequately relaxed. This may require additional xylazine, ketamine, and valium. Glycerol Guaicolate or “Triple Drip” may also be used if a catheter is in place. A good experienced field anesthetist should be in charge of anesthesia.
2.![]() Roll the horse into dorsal recumbency and untie the hind legs. If the rear legs are flexed with a rope it will be much more difficult to visualize the external inguinal ring. The horse can be stabilized by a handler supporting each forelimb at the shoulder. A large pad for the horse’s head and some attention to the rockiness of the ground will prevent pressure injuries to the patient.
Roll the horse into dorsal recumbency and untie the hind legs. If the rear legs are flexed with a rope it will be much more difficult to visualize the external inguinal ring. The horse can be stabilized by a handler supporting each forelimb at the shoulder. A large pad for the horse’s head and some attention to the rockiness of the ground will prevent pressure injuries to the patient.
3.![]() Place bags, towels, or aluminum foil over the horse’s hind feet to prevent dirt from dropping into the surgical field.
Place bags, towels, or aluminum foil over the horse’s hind feet to prevent dirt from dropping into the surgical field.
4.![]() Do a good surgical prep over the entire inguinal area, including the medial sides of the thighs and from the pubis to the end of the sheath. Place a dry towel or cotton in the sheath to keep the penis out of the way and absorb leaked urine.
Do a good surgical prep over the entire inguinal area, including the medial sides of the thighs and from the pubis to the end of the sheath. Place a dry towel or cotton in the sheath to keep the penis out of the way and absorb leaked urine.
5.![]() Draping in the triangular pattern shown is highly desirable, as there will be instances when it may be necessary to enter the abdominal cavity.
Draping in the triangular pattern shown is highly desirable, as there will be instances when it may be necessary to enter the abdominal cavity.
6.![]() Surgeon and assistant must scrub their hands and wear gloves. Sterile sleeves for the surgeon will also allow entry into the abdomen in the rare instances where that is necessary.
Surgeon and assistant must scrub their hands and wear gloves. Sterile sleeves for the surgeon will also allow entry into the abdomen in the rare instances where that is necessary.
7.![]() The surgeon kneels directly behind the patient with the assistant in front of the leg on the side to be explored.
The surgeon kneels directly behind the patient with the assistant in front of the leg on the side to be explored.
8.![]() Palpate the external inguinal ring as above, just to be sure that the testis is not inguinal and to identify the incision site.
Palpate the external inguinal ring as above, just to be sure that the testis is not inguinal and to identify the incision site.
9.![]() Make an incision directly over the external inguinal ring and parallel to it. The incision should be about 1½ times the length of the palpable slit that is the external ring and should be extended no deeper than the dermis. The remaining dissection to find the external inguinal ring is done bluntly with the fingers. Injury to large vessels in this region will make visualization very difficult. As the external inguinal ring is dissected out, the assistant uses fingers or retractors to open the incision and allow visualization. A large self-retaining retractor can be used, but is less adaptable than an assistant.
Make an incision directly over the external inguinal ring and parallel to it. The incision should be about 1½ times the length of the palpable slit that is the external ring and should be extended no deeper than the dermis. The remaining dissection to find the external inguinal ring is done bluntly with the fingers. Injury to large vessels in this region will make visualization very difficult. As the external inguinal ring is dissected out, the assistant uses fingers or retractors to open the incision and allow visualization. A large self-retaining retractor can be used, but is less adaptable than an assistant.
10.![]() The loose areolar connective tissue is bluntly dissected until the white, fibrous external inguinal ring is exposed. A white finger-like projection coming up from the interior of the ring indicates an incomplete cryptorchid covered by the vaginal process. If this is the case, the white membrane (vaginal process) is opened with scissors and the epididymis is pulled into the incision and used as a handle to deliver the testis from the abdomen, as described below.
The loose areolar connective tissue is bluntly dissected until the white, fibrous external inguinal ring is exposed. A white finger-like projection coming up from the interior of the ring indicates an incomplete cryptorchid covered by the vaginal process. If this is the case, the white membrane (vaginal process) is opened with scissors and the epididymis is pulled into the incision and used as a handle to deliver the testis from the abdomen, as described below.
![]()
![]() Prior to birth, the testes begin to shrink. As they shrink, they pull away from the kidney, while they remain very close to the inguinal canal. Just as they added cells to grow in size, they lose cells to shrink. This process leaves each testis somewhat soft and pliable, which allows it to slip through the internal inguinal ring (vaginal ring) and into the inguinal canal.
Prior to birth, the testes begin to shrink. As they shrink, they pull away from the kidney, while they remain very close to the inguinal canal. Just as they added cells to grow in size, they lose cells to shrink. This process leaves each testis somewhat soft and pliable, which allows it to slip through the internal inguinal ring (vaginal ring) and into the inguinal canal.
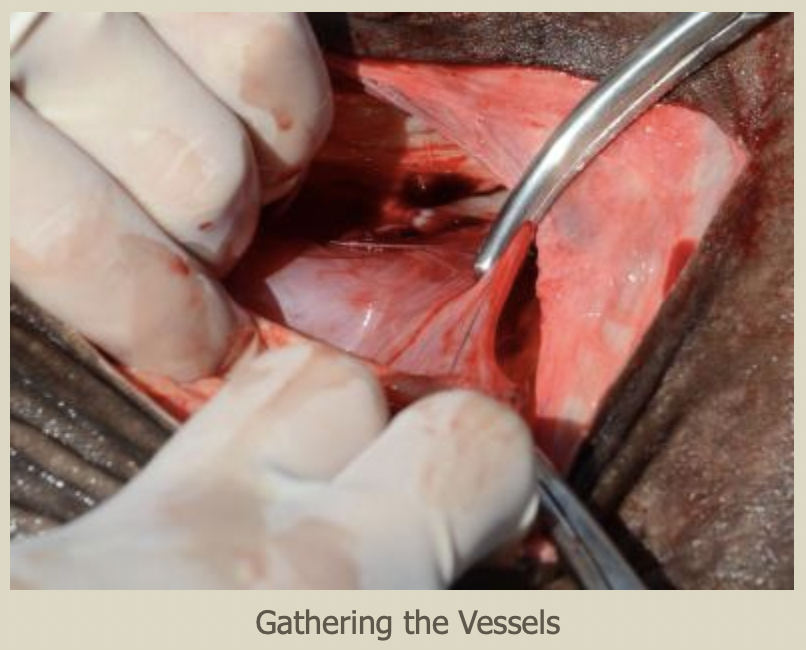
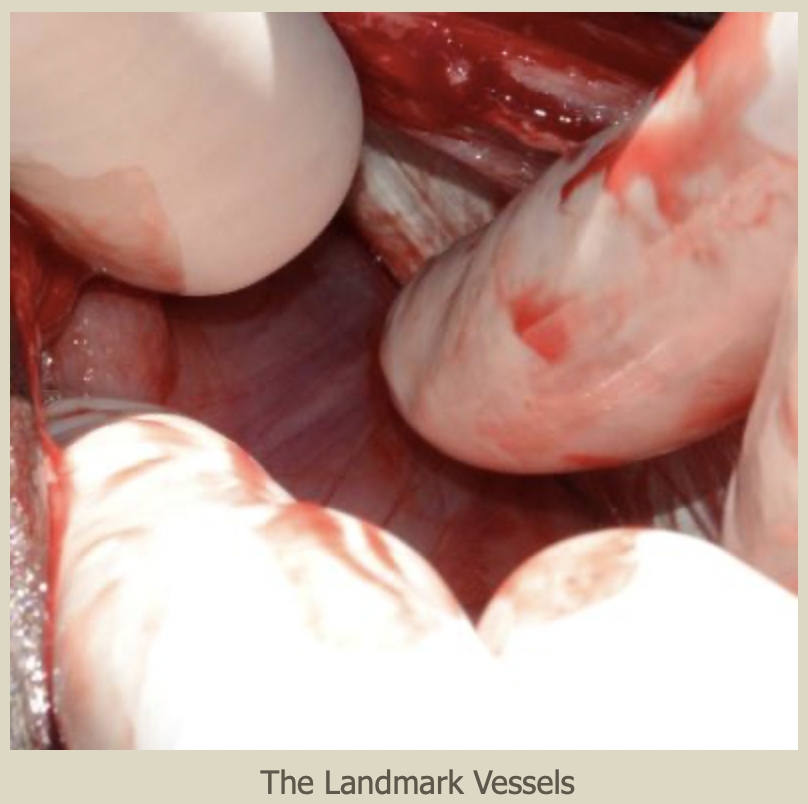
11.![]() More commonly, a group of very thin vessels will be seen going from the surrounding fascia, over the edge of the external inguinal ring and down into the inguinal canal. These vessels may fan out along the entire length of the canal or be in a more discrete bundle. They indicate the tissue that would become the scrotal ligament in a normally descended testis. They should be grasped together, making a bundle.
More commonly, a group of very thin vessels will be seen going from the surrounding fascia, over the edge of the external inguinal ring and down into the inguinal canal. These vessels may fan out along the entire length of the canal or be in a more discrete bundle. They indicate the tissue that would become the scrotal ligament in a normally descended testis. They should be grasped together, making a bundle.
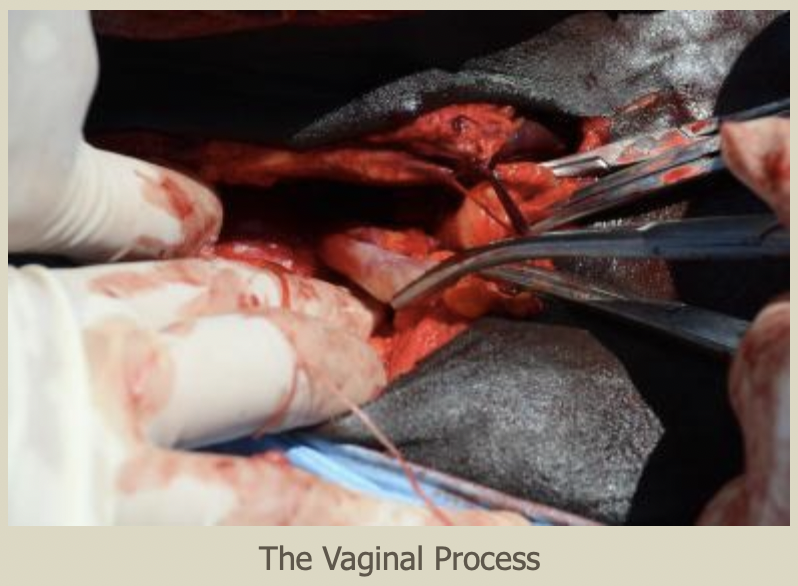
12.![]() Carefully place traction on the bundled vessels (scrotal ligament) to evert the vaginal process through the internal inguinal ring (vaginal ring) and into the inguinal canal. The vaginal process is conical and the tip can be visualized as a small white structure as it passes out of the external inguinal ring. Palpation with an index finger during traction, will establish that the base of the cone is deep inside the inguinal canal. This structure will be more or less easy to mobilize in different horses.
Carefully place traction on the bundled vessels (scrotal ligament) to evert the vaginal process through the internal inguinal ring (vaginal ring) and into the inguinal canal. The vaginal process is conical and the tip can be visualized as a small white structure as it passes out of the external inguinal ring. Palpation with an index finger during traction, will establish that the base of the cone is deep inside the inguinal canal. This structure will be more or less easy to mobilize in different horses.

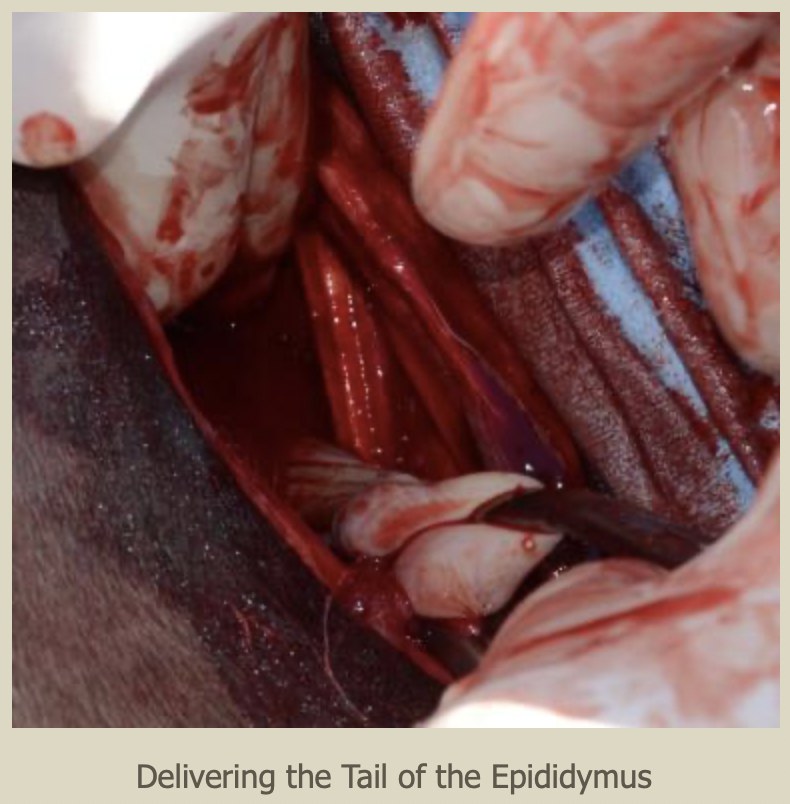
13.![]() Once the vaginal process is identified, it is opened with scissors or the point of a scalpel. Immediately inside the tip of the vaginal process is the ligament of the tail of the epididymis (remnant of the embryonic gubernaculum). This structure is grasped and used to deliver the epididymis through the inguinal canal and into the incision. Firm pressure is required to do this, but it is important not to break and lose the ligament or the epididymis.
Once the vaginal process is identified, it is opened with scissors or the point of a scalpel. Immediately inside the tip of the vaginal process is the ligament of the tail of the epididymis (remnant of the embryonic gubernaculum). This structure is grasped and used to deliver the epididymis through the inguinal canal and into the incision. Firm pressure is required to do this, but it is important not to break and lose the ligament or the epididymis.

14.![]() Using the epididymal structures as a guide and handle traction in placed on the abdominal testis. The object is to deliver the testis through the smallest hole in the vaginal process and without disrupting the internal inguinal ring. A combination of traction, massage with an index finger, and occasionally stretching the vaginal process will deliver nearly every testis, with some patience.
Using the epididymal structures as a guide and handle traction in placed on the abdominal testis. The object is to deliver the testis through the smallest hole in the vaginal process and without disrupting the internal inguinal ring. A combination of traction, massage with an index finger, and occasionally stretching the vaginal process will deliver nearly every testis, with some patience.

15.![]() Once the testis appears through the external inguinal ring, its vessels are ligated as one unit with 2 or 3 Vicryl and cut, along with the vas deferens. The cryptorchid testis and the epididymis are removed and the contralateral testis is castrated.
Once the testis appears through the external inguinal ring, its vessels are ligated as one unit with 2 or 3 Vicryl and cut, along with the vas deferens. The cryptorchid testis and the epididymis are removed and the contralateral testis is castrated.
16.![]() If only minor stretching of the vaginal process is required to remove the cryptorchid testis and the internal inguinal ring was not invaded, the incision is left open to heal by second intention and no further suturing is required. If the testis was larger and more difficult to deliver the inguinal canal can be closed with 2 or 3 Vicryl, by placing one or a few cruciate or simple interrupted stitches across the inguinal canal.
If only minor stretching of the vaginal process is required to remove the cryptorchid testis and the internal inguinal ring was not invaded, the incision is left open to heal by second intention and no further suturing is required. If the testis was larger and more difficult to deliver the inguinal canal can be closed with 2 or 3 Vicryl, by placing one or a few cruciate or simple interrupted stitches across the inguinal canal.
17.![]() Because the inguinal canal in the horse is long and runs up the body wall, the internal inguinal ring cannot be readily identified for suturing. So it is difficult to do a firm closure of the canal if the internal ring has been opened significantly. Further, any suturing in this area should be done with care, due to the large vessels that lay in the fascia around the inguinal canal. If there is concern about the integrity of the closure and possible evisceration, the incision should be tightly packed with a sterile towel and the skin closed in a simple continuous pattern, over the towel. Then in 48-72 hours the sutures and towel are removed. At this time swelling caused by the towel will have closed the canal and granulation has started. This generally requires a second, though brief, anesthesia.
Because the inguinal canal in the horse is long and runs up the body wall, the internal inguinal ring cannot be readily identified for suturing. So it is difficult to do a firm closure of the canal if the internal ring has been opened significantly. Further, any suturing in this area should be done with care, due to the large vessels that lay in the fascia around the inguinal canal. If there is concern about the integrity of the closure and possible evisceration, the incision should be tightly packed with a sterile towel and the skin closed in a simple continuous pattern, over the towel. Then in 48-72 hours the sutures and towel are removed. At this time swelling caused by the towel will have closed the canal and granulation has started. This generally requires a second, though brief, anesthesia.
18.![]() IF the vessels indicating the scrotal ligament cannot be identified; IF the landmarks are broken while attempting to exert traction; or IF the testis is too large to be delivered through the internal inguinal ring: a parainguinal incision can be made, allowing the surgeon to enter the abdomen through a very small incision just next to the inguinal canal.
IF the vessels indicating the scrotal ligament cannot be identified; IF the landmarks are broken while attempting to exert traction; or IF the testis is too large to be delivered through the internal inguinal ring: a parainguinal incision can be made, allowing the surgeon to enter the abdomen through a very small incision just next to the inguinal canal.

19.![]() To utilize the parainguinal incision the assistant retracts the existing skin incision cranially and medially. In this region the internal abdominal oblique muscle is thin, but strong and fibrous. The surgeon selects a site a few inches medial and parallel to the external inguinal ring. A small stab incision is made just though the external muscle sheath. This is extended into the abdomen by using a blunt instrument, such as a the tip of Mayo scissors. The instrument is opened, stretching the incision so that the surgeon can stick two or three fingers into the abdomen.
To utilize the parainguinal incision the assistant retracts the existing skin incision cranially and medially. In this region the internal abdominal oblique muscle is thin, but strong and fibrous. The surgeon selects a site a few inches medial and parallel to the external inguinal ring. A small stab incision is made just though the external muscle sheath. This is extended into the abdomen by using a blunt instrument, such as a the tip of Mayo scissors. The instrument is opened, stretching the incision so that the surgeon can stick two or three fingers into the abdomen.
20.![]() Since the majority of abdominal testes are just next to the internal inguinal ring, the surgeon sweeps laterally and deep to the body wall incision, to palpate and grasp the testis, epididymis, or vas deferens and deliver the testis from the abdomen. The vessels are ligated and cut as above. Closure of the parainguinal incision with sutures in the internal abdominal oblique is a simple matter and very strong. No towel packing or removal is necessary. The skin incision is left open to heal by second intention.
Since the majority of abdominal testes are just next to the internal inguinal ring, the surgeon sweeps laterally and deep to the body wall incision, to palpate and grasp the testis, epididymis, or vas deferens and deliver the testis from the abdomen. The vessels are ligated and cut as above. Closure of the parainguinal incision with sutures in the internal abdominal oblique is a simple matter and very strong. No towel packing or removal is necessary. The skin incision is left open to heal by second intention.
21.![]() In the rare instances in which the abdominal testis cannot be found via the small parainguinal incision described above, the surgeon simply extends the incision made bluntly in the abdominal wall, and, with a sterile sleeve, can explore the entire abdomen, following the decent of the testis from the dorsal body wall. Again, the incision, just large enough to permit the surgeon’s arm is easy to close, once the testis is found and removed.
In the rare instances in which the abdominal testis cannot be found via the small parainguinal incision described above, the surgeon simply extends the incision made bluntly in the abdominal wall, and, with a sterile sleeve, can explore the entire abdomen, following the decent of the testis from the dorsal body wall. Again, the incision, just large enough to permit the surgeon’s arm is easy to close, once the testis is found and removed.
Things Not to Do
- Start surgery before all anesthetic drugs and surgical supplies are immediately ready
- Start surgery before the horse is adequately anesthetized
- Sharply incise structures deep to the skin in the inguinal region. Injury to the large external pudental veins in this region and their branches will result in extreme difficulty in visualizing structures.
- Attempt to find the landmarks around the inguinal canal without good light. Especially avoid having the sun shining in the surgeon’s eyes when working outdoors. A good bright headlamp is a big help.
- Inadequately dissect the fascia from the external inguinal ring. Visualization of the edges of the ring is essential for success. Make sure you can clearly see the ring and if that requires a longer skin incision, make a longer incision.
- Break the remnant of the scrotal ligament: it is the major landmark to the vaginal process. Using large curved Carmault forceps seems to be less traumatic than Ochsners or Kellys. Some surgeons use sponge forces.
- Disrupt the internal inguinal ring. This necessitates suturing the inguinal canal and packing the area with a sterile towel, which must be later removed in a second anesthesia.
A Few Last Points:
- IF the patient’s castration history is unclear and there is scar on the scrotum it may better to postpone the surgery until a serum testosterone or estrone sulfate (depending on the age of the horse) can determine if testicular tissue is present. If this is not possible or if the horse is known to be a hemicastrate, exploration of the inguinal canal as described above will either lead to the cryptorchid testis or it will yield the white fibrous stump of the chord from a removed testis, coming from the external ring into the subcutaneous tissues. Since in Quarter Horse and Paint families an abdominal cryptorchid testis is more likely to be on the left side, it is sensible to approach the left inguinal region first. However, if a chord stump is found on the left side then the right inguinal canal is explored to find the testis.
- Always make sure that you can identify the testis, the head of the epididymis, and the tail of the epididymis before completing a castration. The most common cause of hemicastration (leaving an abdominal testis in the abdomen) is mistaking the tail of the epididymis for a small testis. If you can identify all three structures, you know that you have a complete castration.
- While with adequate sterile technique primary closure of inguinal incisions is possible, the issues of positioning, anesthesia, follow-up, and unrecognized breaks in asepsis make healing an open incision a good alternative in the field. These incisions, even with blunt dissection, seem to heal as rapidly as standard scrotal castrations.
- Remember: have a clear plan and everything AT YOUR FINGERTIPS before you consider starting surgery. This is no time to go looking for equipment and always plan for the procedure being difficult! If you find that you are not ready, allow the horse to recover and plan the procedure for another day.
- Be realistic and prepared to stop the procedure and allow the horse to recover IF:
- You cannot find the important landmarks at the external inguinal ring or you cannot deliver the testis through the inguinal canal and do not want to enter the abdomen
- Light is poor or it is getting dark
- There a serious break in asepsis (ie mud falling into the incision)
- Weather has changed: wind, dust, rain
- The horse is not well anesthetized. This can often happen if an adequate plan of anesthesia was not attained at the start due to inadequate dosage or because the patient was excessively excited. The novice should not attempt this procedure on untrained horses that require IM or oral detomidine to allow venipuncture.
- At any point in the progression of the technique as described above, if the surgeon feels that they cannot successfully complete the procedure. It is far better to stop (given that the abdomen is closed) and allow the horse to recover. Castration is an elective procedure that can be rescheduled when conditions are better. While we cannot always predict complications: “First, do no harm”.
Selected Bibliography:
1.![]() Schumacher J: in Auer, JA, Equine Surgery, 1st ed, W. B. Saunders Co, Philadelphia, 1992, pg. 674-703.
Schumacher J: in Auer, JA, Equine Surgery, 1st ed, W. B. Saunders Co, Philadelphia, 1992, pg. 674-703.
2.![]() Smith JA. The Development and Descent of the Testis in the Horse. Veterinary Annual, 15 th ed., Grunnell CSG and Hill FWG eds. John Wright and Sons Ltd., Bristol, 1975, pgs. 156-161.
Smith JA. The Development and Descent of the Testis in the Horse. Veterinary Annual, 15 th ed., Grunnell CSG and Hill FWG eds. John Wright and Sons Ltd., Bristol, 1975, pgs. 156-161.
3.![]() Bergin WC, Gier HT, et al, A Developmental Concept of Equine Cryptorchidism. Biology of Reproduction, 3, , 1970, 82-90.
Bergin WC, Gier HT, et al, A Developmental Concept of Equine Cryptorchidism. Biology of Reproduction, 3, , 1970, 82-90.
4.![]() Dyce KM, Sack WO, and Wensing CJG. In Textbook of Veterinary Anatomy (Second ed.), WB Saunders Company, Philadelphia, 1996.
Dyce KM, Sack WO, and Wensing CJG. In Textbook of Veterinary Anatomy (Second ed.), WB Saunders Company, Philadelphia, 1996.
5.![]() Wilson DG and Reinertson EL. A Modified Parainguinal Approach for Cryptorchidectomy in Horses An Evaluation in 107 Horses. Veterinary Surgery, 16:1,1987, 1-4.
Wilson DG and Reinertson EL. A Modified Parainguinal Approach for Cryptorchidectomy in Horses An Evaluation in 107 Horses. Veterinary Surgery, 16:1,1987, 1-4.